
 Français
Français 
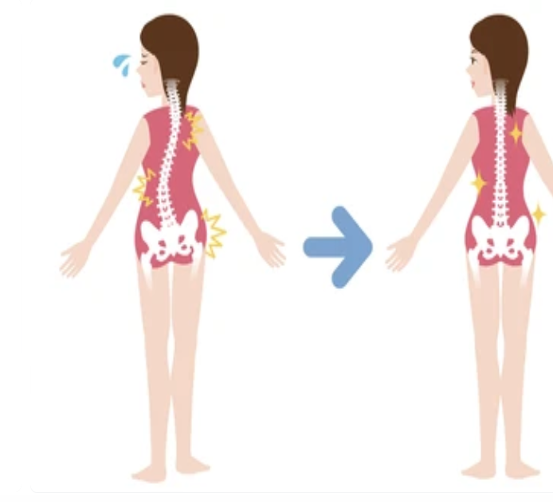
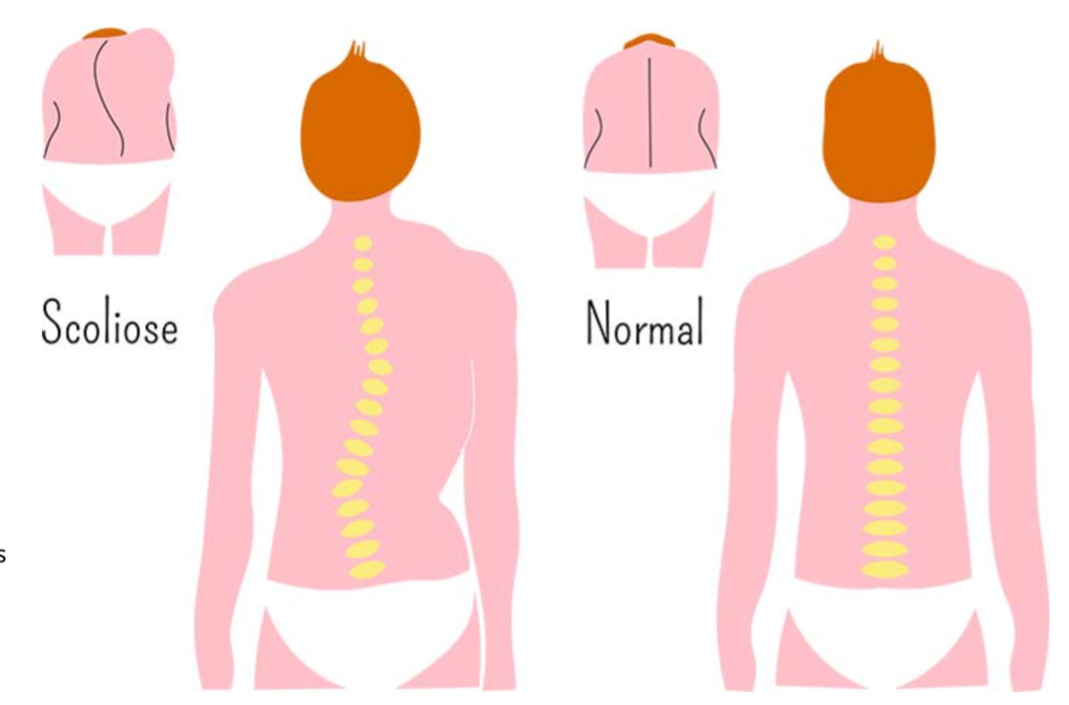
Scoliosis is a lateral deviation of the spine associated with twisting of the spine.
Scoliosis can be manifested by one shoulder being higher than the other, by a prominence in the back, and/or by a lateral translation of the trunk to one side or the other.
The most common form of scoliosis in children is adolescent idiopathic scoliosis (AIS). AIS is defined as scoliosis that begins after the age of 10, and the cause of which remains essentially unknown.
Scoliosis is to be dissociated from the scoliotic attitude which is an apparent scoliosis resulting from a bad posture, without twisting of the vertebrae and without deformation, it can be corrected easily. It does not evolve.
True scoliosis is diagnosed when the angle of deformation exceeds 10°.

The Amplitude of a curvature is measured in degrees by the Cobb method. The angle is measured between the most inclined vertebrae relative to the horizontal on an X-ray taken in a standing position.
Although it most often affects teenagers, scoliosis can also develop in adults. There are several types of scoliosis:
- idiopathic scoliosis, that is to say which is not linked to any other pathology, this is the most frequent
- congenital scoliosis, present from birth
- syndromic scoliosis, of neuromuscular origin
- secondary scoliosis, which as its name suggests is secondary to trauma or another pathology such as cancer for example
- “De novo” scoliosis, linked to spinal degeneration that occurs with age.
Scoliosis can be painless for many years or even a lifetime.
But it still predisposes to have more tension and therefore more pain than the average.
Depending on the severity, scoliosis can lead to pain in the back, or even, in very advanced cases, a loss of respiratory capacity, neurological disorders and/or psychological disorders.
The diagnosis of scoliosis is made primarily by a physical examination of the patient.
In particular, we are looking for the presence (or not) of what is called a humpback, a deformation characteristic of scoliosis which appears in the form of a “bump” when the subject leans forward. The diagnosis is then confirmed by imaging, in particular by frontal and profile X-rays of the spine. Other examinations may be prescribed depending on the severity of the scoliosis but are not absolutely necessary at first.
It is important to monitor the proper development of the spine in children and to detect scoliosis as early as possible before the end of growth for preventive purposes and optimal support.
What can cause scoliosis?
The most common scoliosis is idiopathic scoliosis, that is, scoliosis whose origin is unknown. It usually appears during early childhood or adolescence. Some put forward a hereditary factor, because it is not uncommon to see several members of the same family affected. They represent 70 to 80% of scoliosis.
It can also be caused by a congenital malformation (from birth), a neuromuscular or bone disease. This is called secondary scoliosis.
Bad postures, carrying a too heavy school bag are not involved in the occurrence of scoliosis. These factors can, however, aggravate an already present scoliosis.
Scoliosis is not always diagnosed at an early stage because it does not cause any particular pain. However, back pain and an observation of the spine can alert parents. The visible sign is a deformation of the spine, an impression of bad posture, a collarbone higher than the other from the front and especially a bump on one side of the back. It is also important to check the length of the legs which can vary from each other.
What are the treatments for scoliosis?
Whatever the stage of the scoliosis, the care is generally multidisciplinary, that is to say that it associates several health professionals: general practitioner, osteopath, surgeon, rheumatologist, physiotherapist…
The main goal of treatment is to limit the progression of scoliosis, and therefore the deformities.
For this, several possibilities depending on the stage of severity:
- for mild scoliosis, with minimal curvature, simple monitoring may suffice, with questioning of treatment if the latter worsens; osteopathy makes it possible to limit the aggravation as well as the symptoms (back pain, scapular pain, etc.).
- for moderate scoliosis, the osteopath can also act at this stage in addition to any orthopedic treatment. Wearing a corset can therefore be recommended in certain cases, in order to limit the development of deformities. It is particularly suitable for progressive scoliosis, especially in children or adolescents. In adults, it is mainly prescribed to limit pain.
- when a certain important stage of deformation of the spine is reached, it is possible to consider surgery.
In terms of pain management in the context of scoliosis, it is possible to use analgesic drug treatments.
Physiotherapy is also recommended to relieve pain related to scoliosis by having several effects, in particular by allowing the spine to maintain a certain mobility, to avoid stiffness, by strengthening the muscles in order to allow the spine to better absorb the constraints, etc.
The special case of adult scoliosis
Although scoliosis is in most cases an adolescent pathology that evolves with growth, it is possible to develop scoliosis in adults, especially from the age of 40/50, with wear and degeneration. bone, cartilaginous, ligamentous structures, etc.
There are 2 main types of scoliosis in adults:
- primary or “de novo” degenerative scoliosis, which generally appears from the age of 40/50 and follows the natural wear and tear of bone, cartilaginous, ligamentous structures… This is the one we will talk about later.
- secondary scoliosis following a pathology.
Several factors may be involved in the development of “de novo” scoliosis:
- bone renewal,
- the resistance of the bone mass,
- lumbar disc wear and loss of curvature,
- muscle fatigue,
- osteoarthritis,
- osteoporosis,
- and others…
The main symptoms of adult scoliosis are pain, irritability, fatigue and imbalance of the head in relation to the pelvis.
In terms of treatment, in adults, it differs little or no different from the treatment of progressive scoliosis in adolescents, the aim of treatment being to relieve symptoms, in particular pain, limit deformations and decompress neurological elements.
To do this, the treatment is based on osteopathy, possible wearing of a corset, physiotherapy and surgery if necessary.

The small particularity of the treatment in adults concerns the corset which, in these cases, is not intended to reduce or limit deformations but rather to relieve the intervertebral discs to limit wear and relieve pain.
The use of surgery is more frequent in adulthood than it is in adolescents.
Osteopathic treatment of scoliosis: why and how?
Osteopathy is a manual therapy that can have very positive effects, not on scoliosis itself and its deformities but on the consequences and the evolution of the latter.
In addition to medical and/or physiotherapy treatment, it can reduce the pain and other symptoms associated with scoliosis and considerably improve the quality of life of the patient who suffers from it.
Your osteopath, after asking you a few questions to ensure that he can take care of you without any danger, will apply himself to reducing the tensions resulting from scoliosis, since the spine, by deforming, puts constrain several structures and cause pain or even functional disorders such as respiratory or digestive disorders, for example.
Osteopathy also makes it possible to restore a certain mobility in the spine, in order to avoid or at least limit the stiffness which can result from deformations and cause pain.
Osteopathy is also beneficial in the treatment of scoliotic postures which are often caused by postural imbalance. These postural attitudes are found in the young adolescent who carries his schoolbag with only one shoulder strap, or who often sits very badly askew at his desk during class hours.

Finally, one of the often-underestimated roles of the osteopath in the management of a pathology, here scoliosis, is to give advice to the patient, particularly in terms of stretching or physical activity and answer questions that patients may have in order to support the management of their pathology as best as possible.
In the young adolescent girl it is important that the scoliosis is taken care of before the first menstruation. The scoliosis for her worsens just before the arrival of the periods and then it will be fixed, therefore with a lesser possibility of intervention for the therapists in its care.
After spine surgery following excessive scoliosis, osteopathy can act on scar adhesions and optimize patient recovery.
Sport can also be part of the treatment, it is preferable to choose a sport that allows to promote a symmetrical development of the musculature, such as swimming.
To conclude, the priority in the context of scoliosis is to take care of it as soon as possible and to consult a health professional in order to set up optimal care during the child’s growth and optimize comfort life for the adult.
Ref :
https://www.clinique-du-dos-bordeaux.fr/fra/les-pathologies/39-scoliose
https://rachis.paris